Pregnancy and Substance Abuse: A Harm Reduction Toolkit
This toolkit was designed to help community providers care for pregnant and parenting people who use drugs in a holistic manner. The kit includes information about stigma reduction, trauma-informed care, and legal services. While the guide was developed IN NY, there are engagement and other information that is useful regardless of location.Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants
SAMHSA supported the development of this guide in 2018 to promote evidence-informed care for pregnant and parenting women who have OUD. It includes modules on prenatal care, postnatal care, infant care, and more.Telehealth in a Post-Pandemic Era: Sustainable Approaches to Support Integrated Care – Test
Viewing Time 1 Hour
Telehealth in a Post-Pandemic Era Sustainable Approaches to Support Integrated Care – Part 2
This interactive virtual workshop is part two of a two-part series to support providers ongoing efforts to implement and sustain innovative models of telehealth following the COVID-19 public health emergency. Topics include best practices to support behavioral health care delivery through telehealth; improving patient engagement through telehealth and DC telehealth policy and priority updates.Medicine and Grief During the COVID-19 Era The Art of Losing
Half of Health Workers Report Burnout Amid COVID-19
Telehealth in a Post-Pandemic Era: Sustainable Approaches to Support Integrated Care – Part 1
https://www.integratedcaredc.com/wp-content/uploads/2021/08/Webinar-Telehealth-in-a-Post-Pandemic-Era-Sustainable-Approaches-to-Support-Integrated-Care.mp4 Webinar This interactive virtual workshop is part one of a two-part series to support providers ongoing efforts...Association of Cannabis Use During Adolescence With Neurodevelopment
Results suggest that cannabis use during adolescence is associated with altered neurodevelopment, particularly in cortices rich in cannabinoid 1 receptors and undergoing the greatest age-related thickness change in middle to late adolescence.TEAMcare An Integrated Multicondition Collaborative Care Program for Chronic Illnesses and Depression
Patients with poorly controlled diabetes, coronary heart disease, and depression have an increased risk of adverse outcomes. In a randomized, controlled trial, we tested an intervention designed to improve disease control outcomes for diabetes and/or heart disease and coexisting depression. Patients with one or more parameters of poor medical disease control (ie, HbA1c ≥8.5, or SBP >140, or LDL >130) and a Patient Health Questionnaire-9 (PHQ-9) ≥10 were randomized to the TEAMcare intervention or usual care (N = 214). This article will describe the TEAMcare health services model that has been shown to improve quality of care and medical and psychiatric outcomes.Using Disease Registries to Improve Your Practice Population’s Health
This webinar focuses on effective strategies for engaging justice-involved populations and ways to support individuals transitioning to communities. The speakers shared case studies to illustrate the ways that providers have managed transitions of care and supported people. This session is approved by the American Academy of Family Physicians for up to 1 AMA Level 1 CME credit.Physician Burnout
The health care environment—with its packed workdays, demanding pace, time pressures, and emotional intensity—can put physicians and other clinicians at high risk for burnout. Burnout is a long-term stress reaction marked by emotional exhaustion, depersonalization, and a lack of sense of personal accomplishment. In recent years, the rising prevalence of burnout among clinicians (over 50 percent in some studies) has led to questions on how it affects access to care, patient safety, and care quality. Burned-out doctors are more likely to leave practice, which reduces patients’ access to and continuity of care. Burnout can also threaten patient safety and care quality when depersonalization leads to poor interactions with patients and when burned-out physicians suffer from impaired attention, memory, and executive function.Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide
“Recovery Speaks”: A Photovoice Intervention to Reduce Stigma Among Primary Care Providers
Preliminary findings are reported from a photovoice intervention, “Recovery Speaks, ”to reduce primary care provider stigma in regard to people with mental illness and addiction.Correlates of Patient-Centered Care Practices at U.S. Substance Use Disorder Clinics
Substance use disorder treatment professionals are paying increased attention to implementing patient-centered care. Understanding environmental and organizational factors associated with clinicians’ efforts to engage patients in clinical decision-making processes is essential for bringing patient-centered care to the addictions field. This study examined factors associated with patient-centered care practices in substance use disorder treatment.Stigma, Discrimination, Treatment Effectiveness, & Policy
Cannabis Use May be Associated with Suicidality in Young Adults
NIH study suggests a link between cannabis use and higher levels of suicidal ideation, plan, and attempt. An analysis of survey data from more than 280,000 young adults ages 18-35 showed that cannabis (marijuana) use was associated with increased risks of thoughts of...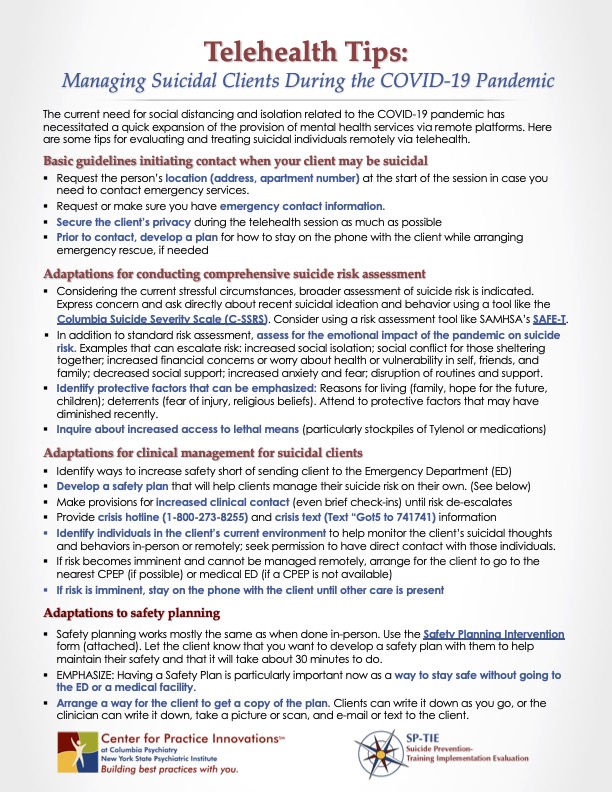
Telehealth Tips: Managing Suicidal Clients During the COVID-19 Pandemic
The current need for social distancing and isolation related to the COVID-19 pandemic has necessitated a quick expansion of the provision of mental health services via remote platforms. This tip sheet provides some tips for evaluating and treating suicidal individuals remotely via telehealth.ASHP Guidelines on Preventing Diversion of Controlled Substances
Controlled substances (CS) diversion in health systems can lead to serious patient safety issues, harm to the diverter, and significant liability risk to the organization. Diversion driven by addiction puts patients at risk of harm, including inadequate relief of pain, inaccurate documentation of their care in the medical record, exposure to infectious diseases from contaminated needles and drugs, and impaired healthcare worker (HCW) performance. In addition to patient harm, there are regulatory and legal risks to the organization, including fraudulent billing and liability for resulting damages, and decreased community confidence in the healthcare system. These guidelines provide a detailed and comprehensive framework to support organizations in developing their CS diversion prevention program (CSDPP) in order to protect patients, employees, the organization, and the community-at-large. Ultimately, each organization is responsible for developing a CSDPP that complies with applicable federal and state laws and regulations but also one that applies technology and diligent surveillance to routinely review process compliance and effectiveness, strengthen controls, and seek to proactively prevent diversion.COVID-19: The Hidden Impact on Mental Health & Drug Addiction
Changes in Adult Alcohol Use and Consequences During the COVID-19 Pandemic in the US
Information for Behavioral Health Providers in Primary Care: Stages of Change: Key Features
Change is not a concrete process, but rather, a fluid process. Individuals tend to move through different “stages of change” in the management of medical problems. These stages include: 1) precontemplation, 2) contemplation, 3) preparation, 4) action, and 5) maintenance.Caring for the Caregiver: A Guide for Physicians
How to Measure Motivational Interviewing Fidelity in Randomized Controlled Trials: Practical Recommendations
Many randomized controlled trials in which motivational interviewing (MI) is a key intervention make no provision for the assessment of treatment fidelity. This methodological shortcoming makes it impossible to distinguish between high- and low-quality MI interventions, and, consequently, to know whether MI provision has contributed to any intervention effects. This article makes some practical recommendations for the collection, selection, coding and reporting of MI fidelity data, as measured using the Motivational Interviewing Treatment Integrity Code. We hope that researchers will consider these recommendations and include MI fidelity measures in future studies.Preliminary Data from the Drug Abuse Warning Network – April 2019-October 2020
Telehealth for the Treatment of Serious Mental Illness & Substance Use Disorders
This guide contains a foreword and five chapters. The chapters stand alone and do not need to be read in order. Each chapter is designed to be brief and accessible to healthcare providers, healthcare system administrators, community members, policymakers, and others working to meet the needs of people at risk for, experiencing, or recovering from SMI and/or SUD. The goal of this guide is to review the literature on the effectiveness of telehealth modalities for the treatment of SMI and SUD, distill the research into recommendations for practice, and provide examples of how practitioners use these practices in their programs.Use of the Family CAGE in Screening for Alcohol Problems in Primary Care
To establish the reliability and validity of the Family CAGE (an acronym indicating Cut down on drinking; Annoyed by complaints about drinking; Guilty about drinking; had an Eye-opener first thing in the morning), a four-item instrument intended to assess family alcohol-related problems.
Counseling Patients in Primary Care: Evidence-Based Strategies
Family physicians spend substantial time counseling patients with psychiatric conditions, unhealthy behaviors, and medical adherence issues. Maintaining efficiency while providing counseling is a major challenge. There are several effective, structured counseling...
Implementing Telemedicine in Primary Care: Learning Lessons From Electronic Health Records
The common narrative is coronavirus disease 2019 happened, payment and policy barriers were quickly lowered, and voila, telemedicine, a technology for which adoption had been slow over the past decade, is, within a matter of months, in widespread and successful use. Fait accompli. On to this narrative has been grafted the hopes that telemedicine will solve other persistent problems, particularly in primary care.Implementing Care for Alcohol & Other Drug Use in Medical Settings An Extension of SBIRT
This change guide is designed to assist primary care clinicians and leaders to integrate care for patients with unhealthy alcohol and/or other drug use into routine medical care. As behavioral health care is increasingly integrated into medical settings, especially primary care, the focus is often on depression and anxiety. Care for alcohol and/or other drugs is often omitted or minimized, likely reflecting: stigma, lack of workforce training/education, and the traditional separation of care for alcohol and other drugs from traditional health care (e.g., primary care, emergency care, and behavioral health, etc.). This guide expands on and updates the widely recognized model of Screening, Brief Intervention, and Referral to Treatment (SBIRT).
Strategies to Encourage Home & Community-Based Care through Value-Based Contracting in Managed Care
This primer examines the financial and policy levers available to states to encourage MCOs to provide care in-home and community-based settings.IBHA Recommended Measures to Assess Behavioral Health Integration in Primary Care
IBHA recommends that health systems, insurance plans, and others looking to measure progress toward integrating behavioral health in primary care use the 2017 PCPCH Standard 3.C.3 as the integration metric of choice. At the system level, IBHA concurs that measuring practice-level progress toward adopting excellent integrated care delivery models in the most meaningful way to affect system change.Fighting Back Against the Stigma of Addiction
Untreated drug and alcohol use contributes to tens of thousands of deaths every year and affects the lives of many more people. We have effective treatments, including medications for opioid and alcohol use disorders, that could prevent a significant number of these deaths, but they are not being utilized widely enough, and people who could benefit often do not even seek them out. One important reason is the stigma around those with addiction.Common Comorbidities with Substance Use Disorders Research Report
When two disorders or illnesses occur in the same person, simultaneously or sequentially, they are described as comorbid. Comorbidity also implies that the illnesses interact, affecting the course and prognosis of both.1,2 This research report provides information on the state of the science in the comorbidity of substance use disorders with mental illness and physical health conditions.Words Matter: Terms to Use and Avoid When Talking About Addiction
This handout offers background information and tips for providers to keep in mind while using person-first language, as well as terms to avoid to reduce stigma and negative bias when discussing addiction. Although some language that may be considered stigmatizing is commonly used within social communities of people who struggle with substance use disorder (SUD), clinicians can show leadership in how language can destigmatize the disease of addiction.Advancing Integrated Mental Health Solutions – Collaborative Care Resources
Collaborative Care (CoCM) is a specific type of integrated care developed at the University of Washington that treats common mental health conditions such as depression and anxiety that require systematic follow-up due to their persistent nature. Based on principles of effective chronic illness care, Collaborative Care focuses on defined patient populations tracked in a registry, measurement-based practice, and treatment to target. Trained primary care providers and embedded behavioral health professionals provide evidence-based medication or psychosocial treatments, supported by regular psychiatric case consultation and treatment adjustment for patients who are not improving as expected.Promoting Culturally & Linguistically Effective Screening Techniques
This module discusses the importance of employing culturally and linguistically effective strategies when r conducting screening and assessments.Staff Wellness & Support Strategies
This module seeks to highlight strategies that may support staff wellness and retention.Why Taking Vitals is so Important
This is a brief video explaining the importance of taking vital signs within a behavioral health setting.Addressing Burnout and Resilience
Burnout is common in healthcare and has increased during the Covid 19 pandemic. This brief presentation defines burnout and it's consequences. Building resilience is a strategy to reduce and prevent burnout. The presentation defines resilience and provides tips in increase personal resilience and organizational resilience.Adolescent Screening for Substance Use Disorders
Adolescents are at the highest risk for experiencing health problems related to substance use. This resource provides an overview of screening adolescents for substance use disorders including assessments and tips.