This tool helps FQHCs understand all of the various VBC elements that are encompassed in a model or program and can impact performance and hence are important consideration in the contract analysis. It provides the considerations, but also guidance on how to approach them and what may be favorable or unfavorable terms within a contract, depending on the scenario and LAN category.
Description: This resource emphasizes the importance of understanding a patient population for successful VBP and provides a foundational understanding of the key considerations in population assessment. Download the Tool
Description: This resource serves as a gap assessment for providers and a roadmap for the needed infrastructure to succeed in advanced value-based models. As providers transition from value-based payment models centered around quality performance to models with...
Description: This resource describes the competencies that providers must systematically master to thrive within each Health Care Payment Learning Action Network (LAN) category. At the very least, all alternative payment models (APMs) necessitate providers to achieve...
Description: This resource serves as a comprehensive guide, offering a step-by-step process for the creation of an integrated and comprehensive quality strategy. The strategy’s core components are thoroughly examined, encompassing population health outcomes and...
This resource is designed to assist leaders in introducing and educating staff about value-based payment (VBP) and value-based care, with a strong emphasis on leadership’s unwavering commitment to the program’s success. Achieving success in VBP arrangements hinges on garnering the full commitment of your workforce and ensuring their continuous participation in VBP activities. The materials provided offer valuable techniques for actively engaging your workforce in the development, implementation, and diligent monitoring of the VBP program.
Description: This resource introduces an initial approach for creating accountable and outcome-driven partnerships spanning the network of healthcare and community-based providers, all geared towards enabling comprehensive, whole-person care. The central focus is on...
This resource covers the development of a value proposition, a compelling statement or proposition that outlines the unique benefits and value that a healthcare provider or organization offers to payers, service recipients, and other stakeholders. A well-crafted value proposition helps healthcare providers and organizations communicate their unique strengths and advantages to payers and patients, ultimately driving engagement, partnerships, and success in value-based payment models.
This resource provides contracting tools to support value-based payment arrangements, beginning with a description of the components of legally enforceable contracts and the legal terms generally found in such contracts. The materials describe key legal considerations for arrangements between providers, which will assist providers in identifying and navigating potential legal issues. Recommendations are offered on how to address legal risks through the purchase of insurance, managing contracts throughout the contracting lifecycle, and negotiating contracts with other organizations.
Description: This resource provides strategies for cultivating a strong relationship with a Managed Care Organization (MCO) when entering into a value-based purchasing agreement. It provides insights into what the payer values and pinpoints measurable outcomes that...
Description: This resource assists providers in understanding the transition from value-based arrangements, which were previously constructed solely on the achievement of quality metrics, to models now grounded in the total cost of care. It furnishes providers with a...
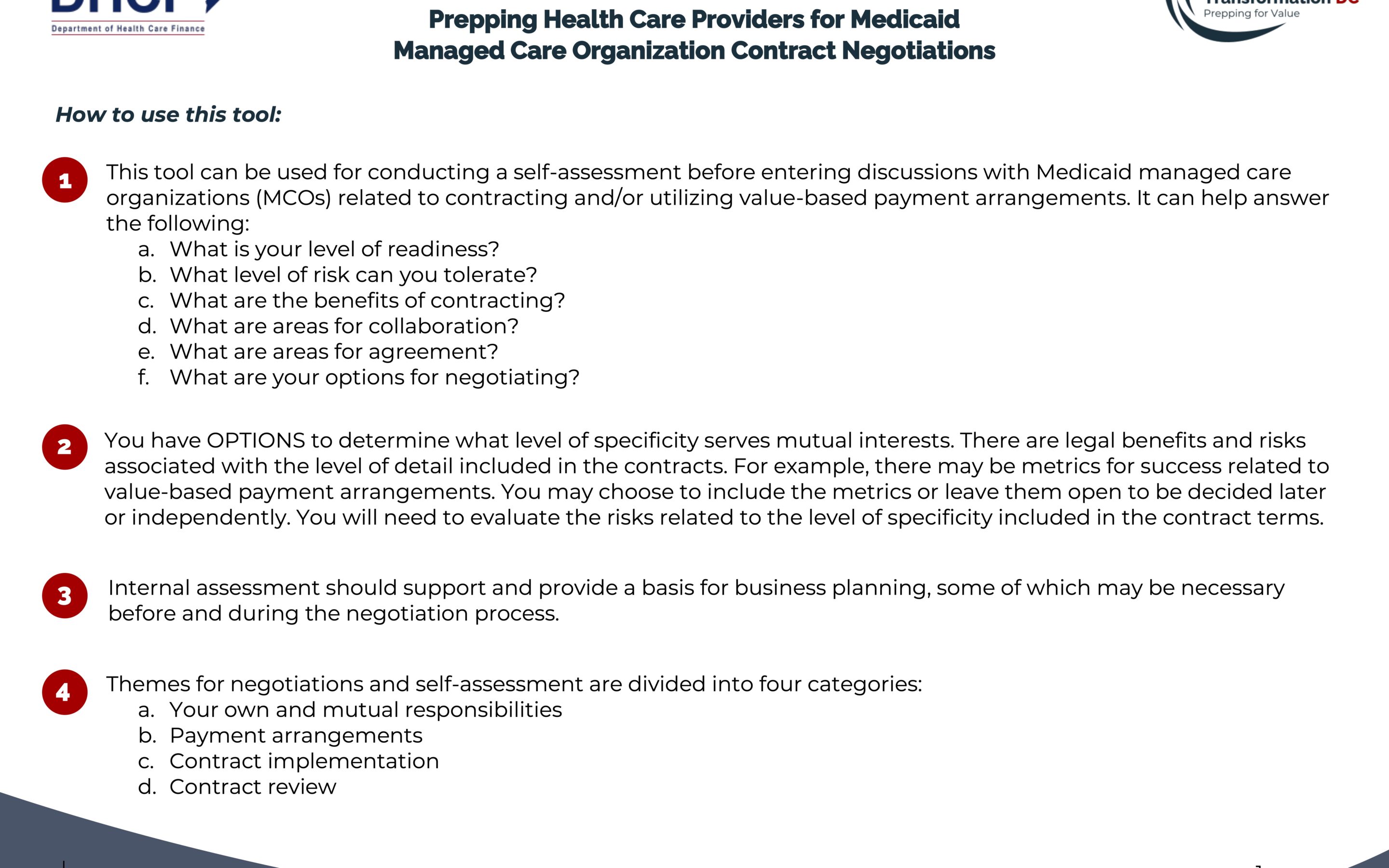
This is a self-assessment tool intended to help health care providers plan for negotiations around proposed managed care contracts. The tool can be used for internal conversations to analyze key terms, develop strategic direction, and set priorities for approaching negotiations. This tool can help providers determine if they are ready to contract, what level of risk they can tolerate, and what areas to focus on in negotiations.
Valuable Revenue Cycle Tip of the Week #7 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #6 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #5 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #4 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #3 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #2 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
Valuable Revenue Cycle Tip of the Week #1 is one of the FREE resources provided by Rev-Up DC, sponsored by the Department of Health Care Finance (DHCF). to help DC Medicaid Behavioral Health providers transition to participating in the Managed Care contracts.
This one-page self-assessment can be utilized before individual or group MAT appointments; this tool aligns with ASAM criteria allowing the provider to plan for the current session and to aid in treatment planning. With a slight modification, this could also be used by persons not on MAT in preparation for individual or group appointments for substance use disorders. Critical questions required for all telehealth appointments are reviewed, such as the address and phone number where the person can be reached today.
The front of this handout reviews what providers need to know, do and have a plan for prior to individual or group telehealth sessions. The back of the handout reviews important features of Zoom (TM) for those staff using Zoom (TM) as a platform for delivering telehealth sessions.
This one-page handout is designed for busy outpatient providers who wish to start a patient on buprenorphine but need guidance on what to do before, important things not to forget when starting, how to monitor patients on buprenorphine, what to do if the patient is or is not doing well and duration of treatment.
This one-page handout will help patients understand when they will start buprenorphine, based on the last time they used opioids and their current level of symptoms. It describes how to take buprenorphine in order for it to help with cravings and withdrawal symptoms, what dose of medication to take when starting and afterwards, and other important information about buprenorphine.
This Clinical Guide provides comprehensive, national guidance for optimal management of pregnant and parenting women with opioid use disorder and their infants. The Clinical Guide helps healthcare professionals and patients determine the most clinically appropriate action for a particular situation and informs individualized treatment decisions.
This worksheet guides the clinician and person receiving services in following the seven steps of problem-solving:
Identifying the problem
Describing the goal
Brainstorming solutions
Evaluating the pros and cons for each potential solution
Choosing the preferred solution
Creating a detailed action plan
Evaluating the outcome.
This patient-facing handout reviews basic steps for meditation, deep breathing, progressive muscle relaxation, and imagery. This can be used when explaining stress reduction techniques to patients.
Results suggest that cannabis use during adolescence is associated with altered neurodevelopment, particularly in cortices rich in cannabinoid 1 receptors and undergoing the greatest age-related thickness change in middle to late adolescence.
Patients with poorly controlled diabetes, coronary heart disease, and depression have an increased risk of adverse outcomes. In a randomized, controlled trial, we tested an intervention designed to improve disease control outcomes for diabetes and/or heart disease and coexisting depression. Patients with one or more parameters of poor medical disease control (ie, HbA1c ≥8.5, or SBP >140, or LDL >130) and a Patient Health Questionnaire-9 (PHQ-9) ≥10 were randomized to the TEAMcare intervention or usual care (N = 214). This article will describe the TEAMcare health services model that has been shown to improve quality of care and medical and psychiatric outcomes.
The health care environment—with its packed workdays, demanding pace, time pressures, and emotional intensity—can put physicians and other clinicians at high risk for burnout. Burnout is a long-term stress reaction marked by emotional exhaustion, depersonalization, and a lack of sense of personal accomplishment. In recent years, the rising prevalence of burnout among clinicians (over 50 percent in some studies) has led to questions on how it affects access to care, patient safety, and care quality. Burned-out doctors are more likely to leave practice, which reduces patients’ access to and continuity of care. Burnout can also threaten patient safety and care quality when depersonalization leads to poor interactions with patients and when burned-out physicians suffer from impaired attention, memory, and executive function.
Preliminary findings are reported from a photovoice intervention, “Recovery Speaks, ”to reduce primary care provider stigma in regard to people with mental illness and addiction.
Substance use disorder treatment professionals are paying increased attention to implementing patient-centered care. Understanding environmental and organizational factors associated with clinicians’ efforts to engage patients in clinical decision-making processes is essential for bringing patient-centered care to the addictions field. This study examined factors associated with patient-centered care practices in substance use disorder treatment.
The current need for social distancing and isolation related to the COVID-19 pandemic has necessitated a quick expansion of the provision of mental health services via remote platforms. This tip sheet provides some tips for evaluating and treating suicidal individuals remotely via telehealth.
Controlled substances (CS) diversion in health systems can lead to serious patient safety issues, harm to the diverter, and significant liability risk to the organization. Diversion driven by addiction puts patients at risk of harm, including inadequate relief of pain, inaccurate documentation of their care in the medical record, exposure to infectious diseases from contaminated needles and drugs, and impaired healthcare worker (HCW) performance. In addition to patient harm, there are regulatory and legal risks to the organization, including fraudulent billing and liability for resulting damages, and decreased community confidence in the healthcare system. These guidelines provide a detailed and comprehensive framework to support organizations in developing their CS diversion prevention program (CSDPP) in order to protect patients, employees, the organization, and the community-at-large. Ultimately, each organization is responsible for developing a CSDPP that complies with applicable federal and state laws and regulations but also one that applies technology and diligent surveillance to routinely review process compliance and effectiveness, strengthen controls, and seek to proactively prevent diversion.
Change is not a concrete process, but rather, a fluid process. Individuals tend to move through different “stages of change” in the management of medical problems. These stages include: 1) precontemplation, 2) contemplation, 3) preparation, 4) action, and 5) maintenance.
Many randomized controlled trials in which motivational interviewing (MI) is a key intervention make no provision for the assessment of treatment fidelity. This methodological shortcoming makes it impossible to distinguish between high- and low-quality MI interventions, and, consequently, to know whether MI provision has contributed to any intervention effects. This article makes some practical recommendations for the collection, selection, coding and reporting of MI fidelity data, as measured using the Motivational Interviewing Treatment Integrity Code. We hope that researchers will consider these recommendations and include MI fidelity measures in future studies.
This guide contains a foreword and five chapters. The chapters stand alone and do not need to be read in order. Each chapter is designed to be brief and accessible to healthcare providers, healthcare system administrators, community members, policymakers, and others working to meet the needs of people at risk for, experiencing, or recovering from SMI and/or SUD.
The goal of this guide is to review the literature on the effectiveness of telehealth modalities for the treatment of SMI and SUD, distill the research into recommendations for practice, and provide examples of how practitioners use these practices in their programs.